PhD - Education | University of Cambridge - UK

PhD - Economics | Central University - Gujarat
The postnatal period, particularly the first 48 hours after childbirth, represents one of the highest-risk windows for maternal morbidity and mortality, yet it remains the weakest link in India’s maternal healthcare continuum (World Health Organisation, 2014, 2022). This study examines systemic gaps in postnatal care (PNC) in Bihar and Uttar Pradesh, two states with persistently low PNC coverage despite major national initiatives such as Janani Suraksha Yojana (JSY), National Health Mission (NHM), Home-Based Newborn Care (HBNC), and LaQshya. Using three rounds of National Family Health Survey (NFHS-3, NFHS-4, NFHS-5) data, the analysis explores long-term trends, equity patterns, and determinants of PNC through descriptive statistics and logistic regression models.
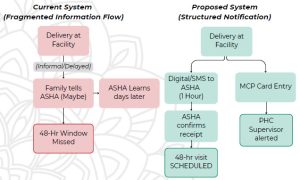
Findings reveal a striking divergence between the rapid rise in institutional deliveries and the comparatively limited progress in maternal PNC. Weak discharge protocols, inadequate facility readiness, broken birth-notification systems, and fragmented frontline worker coordination consistently disrupt continuity of care. Socioeconomic inequalities, caste-based disadvantages, patriarchal constraints, and household infrastructure further shape access. The study highlights that PNC gaps are predominantly supply-side failures that require systemic reform. Strengthening early follow-up mechanisms, data systems, facility readiness, and CHW (Community Health Worker) coordination is essential for improving maternal health outcomes in high-burden states and advancing India’s progress toward SDGs 3, 5, 9, and 10.
The Solutions are structured in two parts. Part A strengthens existing schemes through targeted operational fixes (birth notification protocols, discharge standards, facility-community handovers, and incentive realignment). These interventions address documented system failures at minimal additional cost. Part B introduces a workforce support scheme that recognizes a binding constraint: ASHAs, ANMs, and AWWs cannot deliver quality postnatal care when they are overburdened, irregularly compensated, weakly supervised, and denied career progression. Together, these reforms align Bihar and UP’s maternal health architecture with what evidence shows works.